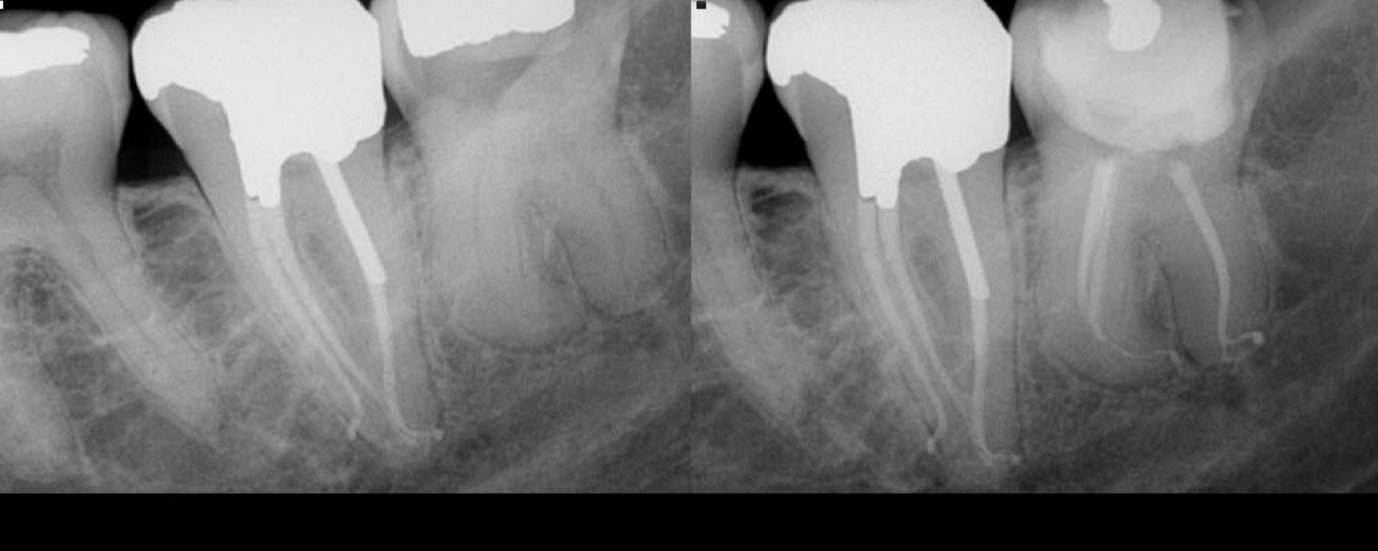
Just the routine endo on a 37 with a C shaped anatomy. Rapid flow technique used for obturation

Online Endodontic Education
Just the routine endo on a 37 with a C shaped anatomy. Rapid flow technique used for obturation

#27 Partial re-treatment of MB2 canal 1) H/O RCT 5yrs bk 2) Exploratory endodontic access revealed a blob of GP in the area where the MB2 should be 3) Pre-op revealed a BF which I missed and I introduced another rotary file into the orifice and it separated as well 4) Both files retrieved with […]

This one had Significantly large irregular canals. Palatal canal obturated with a squirt to get a 3-D fill and the buccal canal with a large POE obturated with MTA at the apical 3rd and back-filled with GP. Done in 2-visits.

Patient reported with pain and swelling in association with #4, Patient was pregnant at the time, treatment was initiated and then long term CaOH2 was placed. MTA truck was downloaded into this blunderbuss anatomy. Vitamin P deficiency ( P*- PCD) – I think I might have contributed to some of it. I had concerns about […]
Somehow i find these premolars canals that splits in the middle 3rd harder to locate and shape than the ones that split in apical. Heat treated NiTi’s come in really handy in these cases.

– Pt age 13yrs old then – IOPA revealed a taurodontic anatomy and a PA lesion in relation to the palatal root. – On access the floor was completely calcified and appeared bleached and ovoid. Managed to localize all canals which were in eccentric locations – I noticed that I had pushed GP outside the […]

#7 referred with a separated file/internal resorption/calcification/apical split > History of trauma and a I/O sinus present Referring doctor had attempted an endo and separated an instrument > Radiograph reveals – Separated file lying horizontal in the internal resorptive defect – A calcified mass of dentin within the resorptive defect – An additional Canal present […]
Treatment of complex third molar. Second molar treated a few years prior.