
#7 referred with a separated file/internal resorption/calcification/apical split
> History of trauma and a I/O sinus present
Referring doctor had attempted an endo and separated an instrument
> Radiograph reveals
– Separated file lying horizontal in the internal resorptive defect
– A calcified mass of dentin within the resorptive defect
– An additional Canal present exiting laterally ?
PA lesion
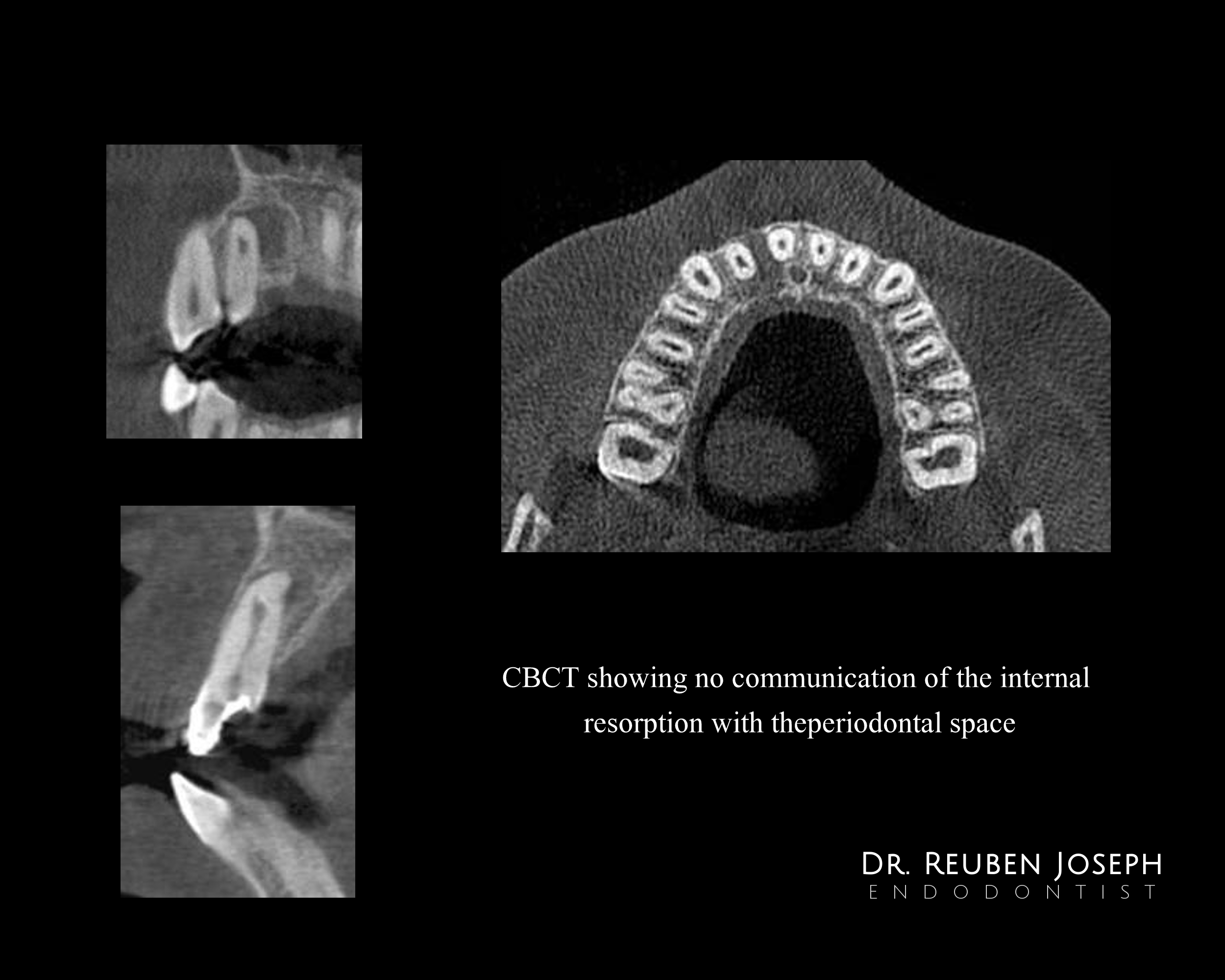
> CBCT findings
No communication of internal resorption externally.
A sharp palatal curve of the root apically.
> Procedure done
– After a little fidgeting around with a U-file the separated instrument straightened up and retrieved
– Unable to establish patency to length due to the calcified mass within the internal resorption and CBCT recommended.
– Calcification drilled out and canals shaped and CaOH dressing (1st visit)
2nd visit – Decided to obturate using the rapid flow technique as the GP kept buckling due to the sharp apical curve and the extra lateral canal had to be filled as well. A blob of thermoplasticized GP placed in the main canal and condensed followed by the same in the lateral canal as well. The rest of the canal back-filled and posts cemented for some root re-inforcement
1yr review showed good progressive healing




What an interesting case! Expertly managed—an impatient clinician could easily screw this case up. Like the deliberate way you handled it!
And I agree, the radiographic finding suggests the area is resolving. Will be nice to see the CBCT in another year.
Beautiful work, Ruben.
gbc
Thanks Dr Gary, I will have a CBCT taken for sure and share it
Retrieving the separated instrument managing internal resorption with calcification and addressing the lateral canal reflect a meticulous approach. The use of CBCT for guidance and the successful 1 year review underscore the effectiveness of your treatment strategy.
Commercial Cleaning Company in Leander TX